


Welcome to part 9 of the ODX Menopause Series. This post focuses specifically on diet and nutrition guidance that can help optimize health before, during, and after menopause. Research on phytoestrogens and herbal medicine is reviewed as well.
The ODX Menopause Series
- Menopause Part 1: A Quick Overview of a Slow Process
- Menopause Part 2: Biology and Physiology of Menopause
- Menopause Part 3: Increased Risk of Disease Associated with Menopause
- Menopause Part 4: Identifying Menopause: Signs and Symptoms
- Menopause Part 5: Laboratory Evaluation of Menopause
- Menopause Part 6: Cardiovascular Risk in Menopause
- Menopause Part 7: Beyond Hormone Testing in Menopause
- Menopause Part 8: Natural Approaches to Menopause
- Menopause Part 9: Diet and Nutrition Intervention in Menopause
- Menopause Part 10: Characteristic of Herbal Derivatives used to Alleviate Menopause Symptoms
- Menopause Part 11: Lifestyle Approaches to Menopause
- Menopause Part 12: The National Institute on Aging Addresses Hot Flashes
- Menopause Part 13: Hormone Replacement Therapy (HRT) in Menopause
- Menopause Part 14: North American and European Guidelines for Hormonal Management of Menopause
- Menopause Part 15: Bioidentical Hormone Therapy
- Menopause Part 16: Optimal Takeaways for Menopause
- Optimal The Podcast - Episode 10
Nutrient insufficiency is a chronic issue globally and is highlighted in the Dietary Guidelines for Americans despite the perceived affluence of the United States. Commonly under-consumed nutrients in women of child-bearing age include calcium, choline, dietary fiber, magnesium, potassium, iron, and vitamins A, C, D, and E. Wisdom does not always come with age. Perimenopausal and menopausal women also have intakes that fall significantly short of estimated average requirements (EARs), including calcium, magnesium, and vitamins A, D, and E. Those with the lowest intake of folate, vitamin D, B12, and DHA had the lowest blood levels of these nutrients as well. [1]
Serum levels of nutrients and their metabolites provide valuable insight into nutrient bioavailability and nutrition status and should be incorporated into a comprehensive health assessment for pre- and postmenopausal women. Dietary supplementation can and should fill in the gaps for consistently insufficient intake or impaired absorption. Supplementation is also associated with better health and lifestyle choices.
An in depth review of 19 studies revealed that a greater intake of unprocessed foods, vegetables, and whole grains was associated with less severe vasomotor, somatic, urogenital, and psychological symptoms. Sleep quality was also improved. On the other hand, increased severity of symptoms was associated with increased intake of processed foods, sugar, and saturated fats. These results are consistent with the concept that a healthy diet contributes to healthy physiology and metabolism.[2]
Prudent guidelines for menopausal women include:[3]
- Antioxidants from plant-based foods
- Almonds, artichokes, blackberries, blueberries, sour cherries, chokeberry, dark chocolate, cloves, cranberries, coffee, grape juice, pomegranate juice, pecans, raspberries, spinach, strawberries, walnuts, spices, red wine (moderation).
- Omega-6s from seeds, nuts
- Omega-3s from flax, fish, seafood
- Herring, mackerel, sardines, salmon, trout, toothfish.
- Phytonutrients
- Allicin found in garlic, chives, leeks, onions
- Capsaicin found in hot peppers
- Carotenoids including beta-carotene, lycopene, lutein
- Curcumin found in turmeric
- Flavonoids found in berries, black and green tea, celery, citrus fruit, olives, onions, oregano, purple grape juice, soybeans, vegetables, whole wheat, wine (in moderation)
- Genistein and daidzein isoflavones found in soybeans, soy flour, soymilk, tofu, textured vegetable protein, legumes
- Indole organosulfur compounds found in cruciferous vegetables including broccoli, Brussels, sprouts, cabbage, cauliflower, horseradish, mustard greens, kale
- Isothiocyanate organosulfur compounds from cruciferous vegetables
- Monoterpenes from citrus peels and oils
- Phenolic acids from coffee beans, apples, blueberries, cherries, grapes, oranges, pears, prunes, oats, potatoes, soybeans
- Resveratrol found in red wine, peanuts, grapes, raspberries
- Saponins found in soybeans, alfalfa and other sprouts, green vegetables, potatoes, tomatoes
- Tannins found in black-eyed peas, grapes, lentils, wine, tea
- Probiotics
- Protein intake of 1-1.2 g/kg
Mediterranean diet
The Mediterranean diet is a good example of a healthy foundation for optimal nutrition. The European Menopause and Andropause Society position statement strongly supports the Mediterranean diet for menopausal health and management and provides the following position paper:[4]
The Mediterranean diet is a non-restrictive dietary pattern common in the olive-
growing areas of the Mediterranean basin. It may improve vasomotor symptoms, cardiovascular risk factors such as blood pressure, cholesterol and blood glucose levels, as well as mood and symptoms of depression. Long-term adherence may: improve cardiovascular risk and events, and death; improve bone mineral density; prevent cognitive decline; and reduce the risk of breast cancer and all-cause mortality
An updated, more environmentally-friendly Mediterranean Diet Pyramid addresses human and environmental health. The update strongly emphasizes decreased consumption of red meat and bovine dairy productions, and increased consumption of legumes and sustainably grown plant-based foods.[5]

Serra-Majem, Lluís et al. “Updating the Mediterranean Diet Pyramid towards Sustainability: Focus on Environmental Concerns.” International journal of environmental research and public health vol. 17,23 8758. 25 Nov. 2020, doi:10.3390/ijerph17238758 This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Supplementation[6]
- Vitamin D supplementation in deficient menopausal women reduced hyperglycemia, hypertriglyceridemia, and overall metabolic syndrome profile.
- Vitamin E supplementation of 800 IU per day may reduce hot flushes, improve sleep quality, and relieve vaginal atrophy.
- Micronutrient supplementation with B vitamins, vitamin C, magnesium, zinc, and essential fatty acids may reduce stress and anxiety in menopause.
- Polyphenols from hops or grapeseed, and mussel extracts may relieve vasomotor and other menopausal symptoms.
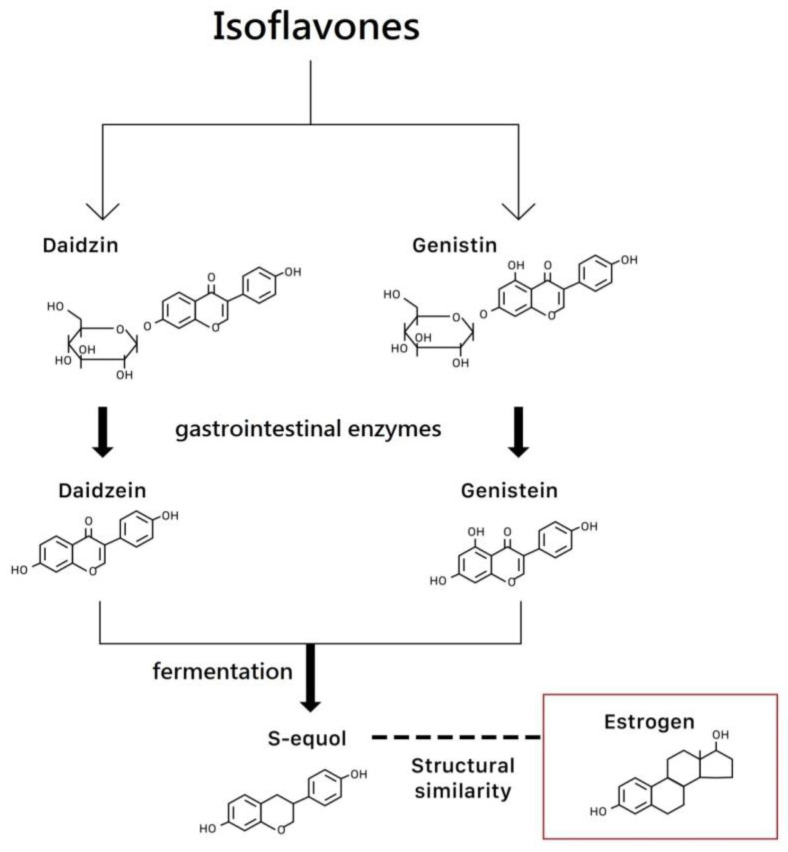
Phytoestrogens
Phytoestrogens are compounds found in plants that can have an estrogen-like effects in the body. Isoflavones act as phytoestrogens and can be found in soybeans (genistein and daidzein), red clover, and alfalfa. Lignans found in fruits, vegetables, whole grains, and flax seeds, also act as phytoestrogens. Because of the nature of their receptor-based mechanisms, phytoestrogens exert estrogenic and antiestrogenic effects and ultimately are considered safe and possibly protective against hormone-related cancers.[7]
Isoflavones have shown promise in reducing vasomotor symptoms, moderating lumbar spine loss, and improving bone mineral density.[8] Though not as clinically effective as hormone replacement therapy, phytoestrogens may be an option for women seeking a non-hormonal approach to menopause.
Chen, Li-Ru, and Kuo-Hu Chen. “Utilization of Isoflavones in Soybeans for Women with Menopausal Syndrome: An Overview.” International journal of molecular sciences vol. 22,6 3212. 22 Mar. 2021, doi:10.3390/ijms22063212 This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Isoflavones can bind to estrogen receptors with a weak affinity for ER-alpha (predominantly found in the breast and uterus), and a stronger affinity for ER-beta (predominantly found in bone, urogenital tract, and the cardiovascular system). Systematic review reveals that though the mechanism of action for isoflavones in menopause is not completely understood, supplementation is beneficial for many individuals. The NAMS recommends a trial of isoflavones of at least 50 mg per day for 12 weeks with a continuation of therapy if benefits are significant.[9]
One study of 20 postmenopausal women found that daily intake of 69 milligrams of soy isoflavones increased low normal levels of SHBG from 55.5 nmol/L to 64.2 nmol/L in women maintaining a serum isoflavone level of at least 0.6 umol/L.[10]
Systematic review and meta-analysis comprising 2305 postmenopausal women in 29 studies evaluated the effect of soy isoflavone extract and isoflavone-rich soy protein isolate on serum lipids. Analysis demonstrated a significant reduction in total cholesterol and significant increase in HDL-C. Reductions in LDL-C and triglycerides were also observed.[11]
A double-blind, placebo-controlled trial of 78 symptomatic menopausal women evaluated the effects of 190 mg of a combined soy and hop isoflavone extract on menopausal symptoms. Results revealed a 20.6 point improvement in symptoms score with treatment compared to 14.8 points in the placebo group. These women experienced significant improvement in pain, palpitations, fatigue, paresthesia, and vaginal dryness.[12]
Herbal Medicine
Herbal medicine has been used by humans for thousands of years without knowing the full mechanism of action, though that does not negate their effectiveness. The following uses have been identified for menopausal symptoms: [13]
- Actaea racemose Hot flashes, insomnia, irritability, musculoskeletal pain
- Gingko biloba: Attention deficits
- Panax ginseng: Depression, sexual function, sleep disorders
- Valerian officinal Anxiety, dysmenorrhea, hot flashes, sleep disorder
Mounting research reveals herbal formulas can effectively address menopausal symptoms as well as improve metabolic profiles.
A 2017 literature review of clinical trials revealed that several medicinal plants were effective in addressing acute menopausal symptoms including:[14]
- Alfalfa
- Black cohosh
- Black cumin
- Evening primrose
- Fennel
- Fenugreek
- Ginkgo biloba
- Glycine soja
- Hypericum perforatum (St. John’s wort)
- Lemon balm
- Licorice
- Panax ginseng
- Passiflora incarnata
- Pimpinella anisum
- Red clover
- Sage
- Valerian
- Vitex
In one randomized, double-blind, placebo-controlled trial of 111 postmenopausal women, 12 weeks of supplementation with black cohosh, chasteberry, evening primrose oil, and soy isoflavones significantly reduced hot flashes, sweating, sleep issues, irritability, and depressed mood. Although hormone levels remained similar between subjects and controls, levels of CRP, LDL-cholesterol, and triglycerides were significantly reduced in the active group.[15]
Meta-analysis and review of 19 randomized controlled studies revealed that Chinese herbal medicine reduced menopausal symptoms effectively even though no statistically significant differences in hormone levels occurred. The analysis concluded that herbal intervention significantly improved vasomotor symptoms, quality of life, and upper-body peripheral blood flow.[16]
References
[1] Devarshi, Prasad P et al. “Total estimated usual nutrient intake and nutrient status biomarkers in women of childbearing age and women of menopausal age.” The American journal of clinical nutrition vol. 113,4 (2021): 1042-1052. doi:10.1093/ajcn/nqaa392
[2] Noll, P R E S et al. “Dietary intake and menopausal symptoms in postmenopausal women: a systematic review.” Climacteric : the journal of the International Menopause Society vol. 24,2 (2021): 128-138. doi:10.1080/13697137.2020.1828854
[3] Ko, Seong-Hee, and Hyun-Sook Kim. “Menopause-Associated Lipid Metabolic Disorders and Foods Beneficial for Postmenopausal Women.” Nutrients vol. 12,1 202. 13 Jan. 2020, doi:10.3390/nu12010202 This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ().
[4] Cano, Antonio et al. “The Mediterranean diet and menopausal health: An EMAS position statement.” Maturitas vol. 139 (2020): 90-97. doi:10.1016/j.maturitas.2020.07.001
[5] Serra-Majem, Lluís et al. “Updating the Mediterranean Diet Pyramid towards Sustainability: Focus on Environmental Concerns.” International journal of environmental research and public health vol. 17,23 8758. 25 Nov. 2020, doi:10.3390/ijerph17238758
[6] De Franciscis, Pasquale et al. “A Nutraceutical Approach to Menopausal Complaints.” Medicina (Kaunas, Lithuania) vol. 55,9 544. 28 Aug. 2019, doi:10.3390/medicina55090544
[7] Laudisio, Daniela et al. “A practical nutritional guide for the management of sleep disturbances in menopause.” International journal of food sciences and nutrition, 1-15. 30 Nov. 2020, doi:10.1080/09637486.2020.1851658
[8] Chen, Li-Ru, and Kuo-Hu Chen. “Utilization of Isoflavones in Soybeans for Women with Menopausal Syndrome: An Overview.” International journal of molecular sciences vol. 22,6 3212. 22 Mar. 2021, doi:10.3390/ijms22063212 This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ().
[9] Chen, Li-Ru et al. “Isoflavone Supplements for Menopausal Women: A Systematic Review.” Nutrients vol. 11,11 2649. 4 Nov. 2019, doi:10.3390/nu11112649
[10] Pino, A M et al. “Dietary isoflavones affect sex hormone-binding globulin levels in postmenopausal women.” The Journal of clinical endocrinology and metabolism vol. 85,8 (2000): 2797-800. doi:10.1210/jcem.85.8.6750
[11] Baranska, Agnieszka et al. “Effects of Soy Protein Containing of Isoflavones and Isoflavones Extract on Plasma Lipid Profile in Postmenopausal Women as a Potential Prevention Factor in Cardiovascular Diseases: Systematic Review and Meta-Analysis of Randomized Controlled Trials.” Nutrients vol. 13,8 2531. 24 Jul. 2021, doi:10.3390/nu13082531 [R}
[12] Kim, Hye In et al. “Efficacy and Safety of a Standardized Soy and Hop Extract on Menopausal Symptoms: A 12-Week, Multicenter, Randomized, Double-Blind, Placebo-Controlled Clinical Trial.” Journal of alternative and complementary medicine (New York, N.Y.), 10.1089/acm.2021.0027. 16 Aug. 2021, doi:10.1089/acm.2021.0027
[13] Chen, Li-Ru et al. “Isoflavone Supplements for Menopausal Women: A Systematic Review.” Nutrients vol. 11,11 2649. 4 Nov. 2019, doi:10.3390/nu11112649
[14] Kargozar, Rahele et al. “A review of effective herbal medicines in controlling menopausal symptoms.” Electronic physician vol. 9,11 5826-5833. 25 Nov. 2017, doi:10.19082/5826
[15] Rattanatantikul, Teerapong et al. “Efficacy and Safety of Nutraceutical on Menopausal Symptoms in Post-Menopausal Women: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial.” Journal of dietary supplements, 1-15. 17 Dec. 2020, doi:10.1080/19390211.2020.1853648
[16] Li, Mingdi et al. “Chinese herbal formulae for the treatment of menopausal hot flushes: A systematic review and meta-analysis.” PloS one vol. 14,9 e0222383. 19 Sep. 2019, doi:10.1371/journal.pone.0222383


