


Loss of Muscle Means Loss of Function
Sarcopenia is the progressive loss of skeletal muscle mass and strength that can lead to adverse outcomes. It is often associated with aging, loss of functionality, and a decreased quality of life. Sarcopenia is formally recognized as a muscle disease by the World Health Organization (Ren 2022).
Ideally, the assessment of sarcopenia comprises physical measurements of whole-body lean mass, appendicular lean mass, or muscle mass and size. Physical performance measurements can also include grip strength, leg muscle strength, walk speed, or a battery of physical performance tests involving walk speed, chair stands, and balance (Ganapathy 2020). Evaluating nutrition status and blood chemistry is vital to a comprehensive sarcopenia assessment as well.
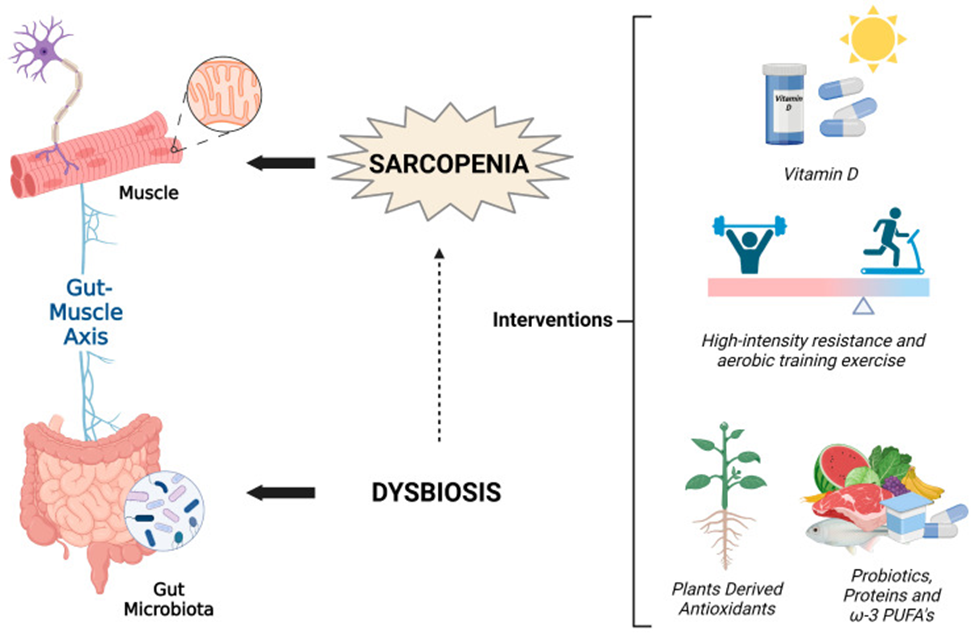
Sarcopenia is influenced by chronic inflammation, oxidative stress, nutrient insufficiency, hormonal changes, gut microbiota imbalances, mitochondrial and autophagy dysfunction, decreased regenerative capacity, loss of skeletal muscle stem cells, ectopic and intermuscular adiposity, and a sedentary lifestyle. Vitamin D insufficiency can directly contribute to sarcopenia as it can cause muscle atrophy, peroxidation of skeletal muscle, impairment of antioxidant enzymes, increased production of mitochondrial reactive oxygen species, and decreased mitochondrial energy production (Agostini 2023).
Functional interventions with the potential to prevent or counteract sarcopenia (Agostini 2023, Ganapathy 2020):
- Alkaline diet
- Antioxidants, including polyphenols, curcumin, and resveratrol
- Dairy products
- Exercise, resistance training, and increased physical activity
- Fruits and vegetables
- Kefir
- Leucine
- Mediterranean-style diet
- Medium-chain fatty acids
- Minerals: calcium, magnesium, potassium, selenium,
- Omega-3 fatty acids
- Polyunsaturated fatty acids
- Prebiotics
- Probiotics
- Protein
- Short-chain fatty acids
- Vitamins: A, B 6, B12, C, D
- Whey protein
Source: Agostini, Deborah et al. “An Integrated Approach to Skeletal Muscle Health in Aging.” Nutrients vol. 15,8 1802. 7 Apr. 2023, doi:10.3390/nu15081802 This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Research suggests that 90-100 grams of protein distributed throughout the day can help reduce the risk of muscle wasting and neurotransmitter depletion, especially in the setting of acute or chronic pain. A higher intake may be indicated depending on weight. Therefore, at least 1 gram of protein per kg body weight is recommended. Neurotransmitters, including serotonin, GABA, and endorphins, are synthesized from the amino acids found in protein. Essential foods to consume include those high in glutamic acid (e.g., eggs, soy, and cod), tryptophan (e.g., milk, dairy foods, and peanuts), and leucine (whey protein). Consumption of ginger and curcumin can also help reduce the pain associated with muscle mass loss (Perna 2020).
Micronutrients are also significant factors to consider when evaluating sarcopenia. Magnesium is essential to preventing loss of muscle mass and function due to its vital role in the body, including protein synthesis, energy production, oxygen uptake, electrolyte balance, glycogen breakdown, fat oxidation, and reduction of C-reactive protein and inflammatory cytokines. Vitamin D also plays a vital role in addressing sarcopenia and musculoskeletal pain, affecting neuromuscular performance, muscle size, and muscle strength (Perna 2020). Vitamins A, B6, B12, C, carotenoids, and omega-3 fatty acids are significant factors in maintaining lean body mass and muscle strength (Ganapathy 2020).
Clinical factors to consider when assessing sarcopenia
Evaluation of sarcopenia should take into account biomarkers that reflect oxidative stress, inflammation, energy metabolism, and hormone balance and can include (Jones 2022):
- Albumin
- Antioxidant capacity
- Bioelectrical impendence analysis
- Bone mineral density
- Cholesterol, total, LDL, HDL
- Creatinine
- CRP
- Cystatin C
- ESR
- Fibrinogen
- Glucose
- HbA1c
- HOMA2
- IL‐6
- Leptin
- MTHFR status
- Oxidative stress markers
- Testosterone, free
- TNF-alpha
- Triglycerides
- Total cholesterol
- Triglycerides
- Vitamin D, 25(OH)D
A cross-sectional study of UK Biobank data from 396,707 subjects found that sarcopenia was associated with various biomarker patterns, including (Petermann-Rocha 2020):
Lower
- IGF-1, albumin, creatinine, and sodium in men and women
- Vitamin D, apolipoprotein A, and apolipoprotein B in men
- Hemoglobin A1C, urea, glucose, testosterone, and total bilirubin in women
Higher
- C-reactive protein, cystatin C, sex hormone-binding globulin, GGT, alkaline phosphatase, total protein, and rheumatoid factor in men and women
- HDL, AST, and direct bilirubin in men
- Phosphate and lipoprotein (a) in women
Sarcopenia Index (serum creatinine/serum cystatin C × 100)
The Sarcopenia Index is based on creatinine and cystatin C. Creatinine is a byproduct of muscle metabolism that the kidneys must excrete. Low levels are associated with low muscle mass. Cystatin C is made by most cells in the body and excreted by the kidneys at a consistent rate; it is less affected by muscle mass. A low sarcopenia index value suggests reduced muscle mass, while a high value is associated with a lower risk of sarcopenia, all-cause mortality, and nutrition risk. A higher sarcopenia index correlated significantly with higher albumin, hemoglobin, body mass index, waist and calf circumference, and hand grip strength in a prospective study of 758 hospitalized patients. Higher sarcopenia index was correlated with a lower triglyceride glucose index which is associated with a lower risk of insulin resistance and cardiometabolic disorders (Ren 2022).
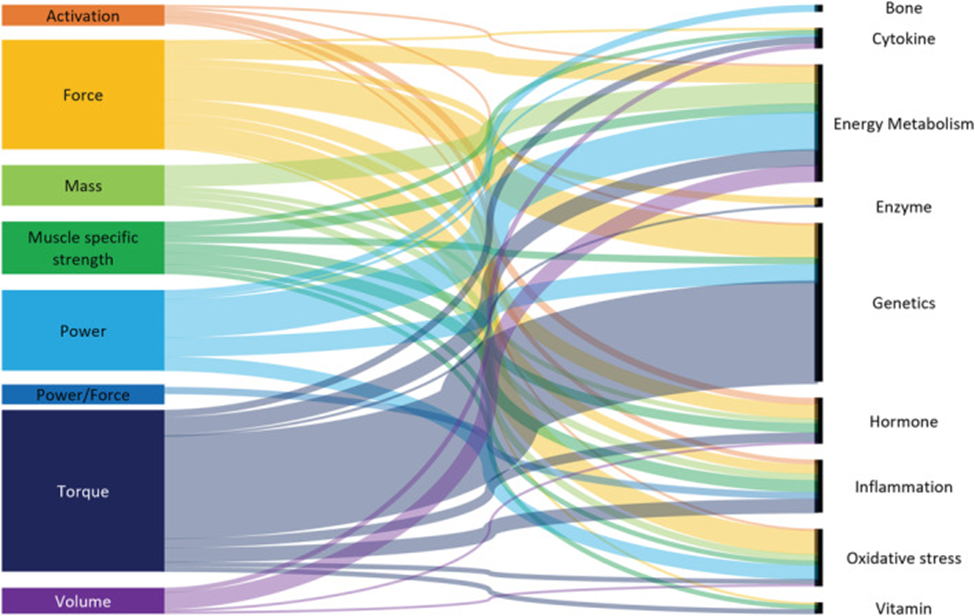
Sankey diagram of lower limb muscle measures and biomarkers
(based on the primary role)
Source: Jones, Rebecca Louise et al. “Biomarkers associated with lower limb muscle function in individuals with sarcopenia: a systematic review.” Journal of cachexia, sarcopenia and muscle vol. 13,6 (2022): 2791-2806. doi:10.1002/jcsm.13064 This is an open access article under the terms of the http://creativecommons.org/licenses/by-nc-nd/4.0/ License
Optimal Takeaways
- Sarcopenia, recognized as a muscle disease by the WHO, is the progressive loss of skeletal muscle mass and strength often associated with aging, loss of functionality, and a decreased quality of life. Its evaluation requires physical measurements, nutrition status assessment, and blood chemistry.
- Numerous factors influence sarcopenia, including chronic inflammation, oxidative stress, nutrient insufficiency, hormonal changes, gut microbiota imbalances, and a sedentary lifestyle. Additionally, Vitamin D insufficiency can directly contribute to sarcopenia.
- Preventive interventions include various nutritional measures such as consuming alkaline diets, antioxidants, dairy products, and certain vitamins and minerals and increasing physical activity. Protein consumption of 90-100 grams distributed throughout the day can help reduce muscle wasting and neurotransmitter depletion.
- Important micronutrients in addressing sarcopenia include magnesium, essential for protein synthesis and energy production, and vitamins A, B6, B12, C, D, carotenoids, and omega-3 fatty acids, which are significant for maintaining lean body mass and muscle strength.
- Assessment of sarcopenia should consider clinical biomarkers reflecting oxidative stress, inflammation, energy metabolism, and hormone balance, such as albumin, creatinine, glucose, and vitamin D, 25(OH)D, among others.
- A cross-sectional study of UK Biobank data discovered patterns in biomarkers associated with sarcopenia, including lower levels of IGF-1, albumin, creatinine, sodium, and higher levels of C-reactive protein, cystatin C, and sex hormone-binding globulin, among others.
- The Sarcopenia Index, based on creatinine and cystatin C, provides insight into muscle mass. A low index suggests reduced muscle mass, while a high value is linked with a lower risk of sarcopenia, all-cause mortality, and nutrition risk. A higher sarcopenia index was correlated with a lower triglyceride glucose index which is associated with a lower risk of insulin resistance and cardiometabolic disorders.
Want to Learn More?
CLICK HERE and listen to more about preserving muscle mass and addressing sarcopenia at Optimal the Podcast with Kathie Swift, MS, RDN, LDN, FAND, EBQ

References
Agostini, Deborah et al. “An Integrated Approach to Skeletal Muscle Health in Aging.” Nutrients vol. 15,8 1802. 7 Apr. 2023, doi:10.3390/nu15081802 This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/
4.0/).
Ganapathy, Aravinda, and Jeri W Nieves. “Nutrition and Sarcopenia-What Do We Know?.” Nutrients vol. 12,6 1755. 11 Jun. 2020, doi:10.3390/nu12061755 This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Jones, Rebecca Louise et al. “Biomarkers associated with lower limb muscle function in individuals with sarcopenia: a systematic review.” Journal of cachexia, sarcopenia and muscle vol. 13,6 (2022): 2791-2806. doi:10.1002/jcsm.13064
Perna, Simone et al. “Evidence-Based Role of Nutrients and Antioxidants for Chronic Pain Management in Musculoskeletal Frailty and Sarcopenia in Aging.” Geriatrics (Basel, Switzerland) vol. 5,1 16. 6 Mar. 2020, doi:10.3390/geriatrics5010016
Petermann-Rocha, Fanny et al. “Biomarkers Profile of People With Sarcopenia: A Cross-sectional Analysis From UK Biobank.” Journal of the American Medical Directors Association vol. 21,12 (2020): 2017.e1-2017.e9. doi:10.1016/j.jamda.2020.05.005
Ren, Chenxi et al. “Sarcopenia Index Based on Serum Creatinine and Cystatin C is Associated with Mortality, Nutritional Risk/Malnutrition and Sarcopenia in Older Patients.” Clinical interventions in aging vol. 17 211-221. 1 Mar. 2022, doi:10.2147/CIA.S351068
Sim, Marc et al. “Creatinine to Cystatin C Ratio, a Biomarker of Sarcopenia Measures and Falls Risk in Community-Dwelling Older Women.” The journals of gerontology. Series A, Biological sciences and medical sciences vol. 77,7 (2022): 1389-1397. doi:10.1093/gerona/glab369


